
Is the Polyvagal Theory over?
Scientific debate since a publication in early 2026 has put into question the groundbreaking neurophysiological theory that has based many somatic practitioners’ work. The creator of the theory himself, though, has refuted some of the criticism. Keep reading for more.
We live in an era of extraordinary neurobiological curiosity. Over the past three decades, advances in brain imaging — from fMRI to EEG — have allowed scientists to observe the living brain in real time, mapping the neural correlates of emotion, memory, decision-making, and even transcendence. This revolution has not stayed confined to laboratories. It has moved into therapy rooms, onto stages, and into meditation centres, reshaping how artists, healers, and spiritual practitioners understand the ancient wisdom they carry.
Researchers revisiting indigenous South American traditions through a neuroscientific lens, for example, have found what they describe as an intuitive neurobiological wisdom embedded in these practices — a recognition that healing is simultaneously physiological and spiritual. Spiritual practices and religious rituals have been around for hundreds of thousands of years, and neurotheology — the field that seeks to explain the biological and neurological processes behind religious experience — has been offering a scientific language for what human communities have been doing intuitively across cultures and millennia.
What makes this moment particularly rich is that neuroscience is not replacing ancestral knowledge — it is, in many cases, confirming it. Research into the intersection of neuroscience and spirituality suggests that integrating neurocognitive strategies with spiritual practices fosters neuroplastic changes in the prefrontal cortex and limbic system, improving executive function and emotion regulation. Meditative practices, for instance, have shown measurable neuroanatomical and neurochemical changes, and their positive impact on mental health is increasingly supported by neurobiological evidence.
For artists and performers, this convergence is especially potent: the rituals of vocal warm-up, breath work, embodied rehearsal, and collective creative flow are no longer merely intuitive — they are biologically legible. Neuroscience has given us a new vocabulary for understanding why the body must be involved in transformation, and why presence, safety, and connection are not soft concepts but physiological states. It is within this broader cultural and scientific moment that theories like the Polyvagal Theory have emerged and flourished.
An epistemological background to the Polyvagal Theory
The triune brain was proposed by US American physician and neuroscientist Paul D. MacLean in the 1960s, and has been largely disputed since the 1970s as a viable scientific theory. As seen in the image below, the trimembered brain elicits a co-evolutionary model of the brain, in which three distinct layers — the reptilian complex, the limbic system, and the neocortex — are thought to have developed sequentially across evolutionary time, each governing increasingly complex behaviour. The reptilian brain handles survival and instinct, the limbic system manages emotion and memory, and the neocortex is responsible for rational thought and language.
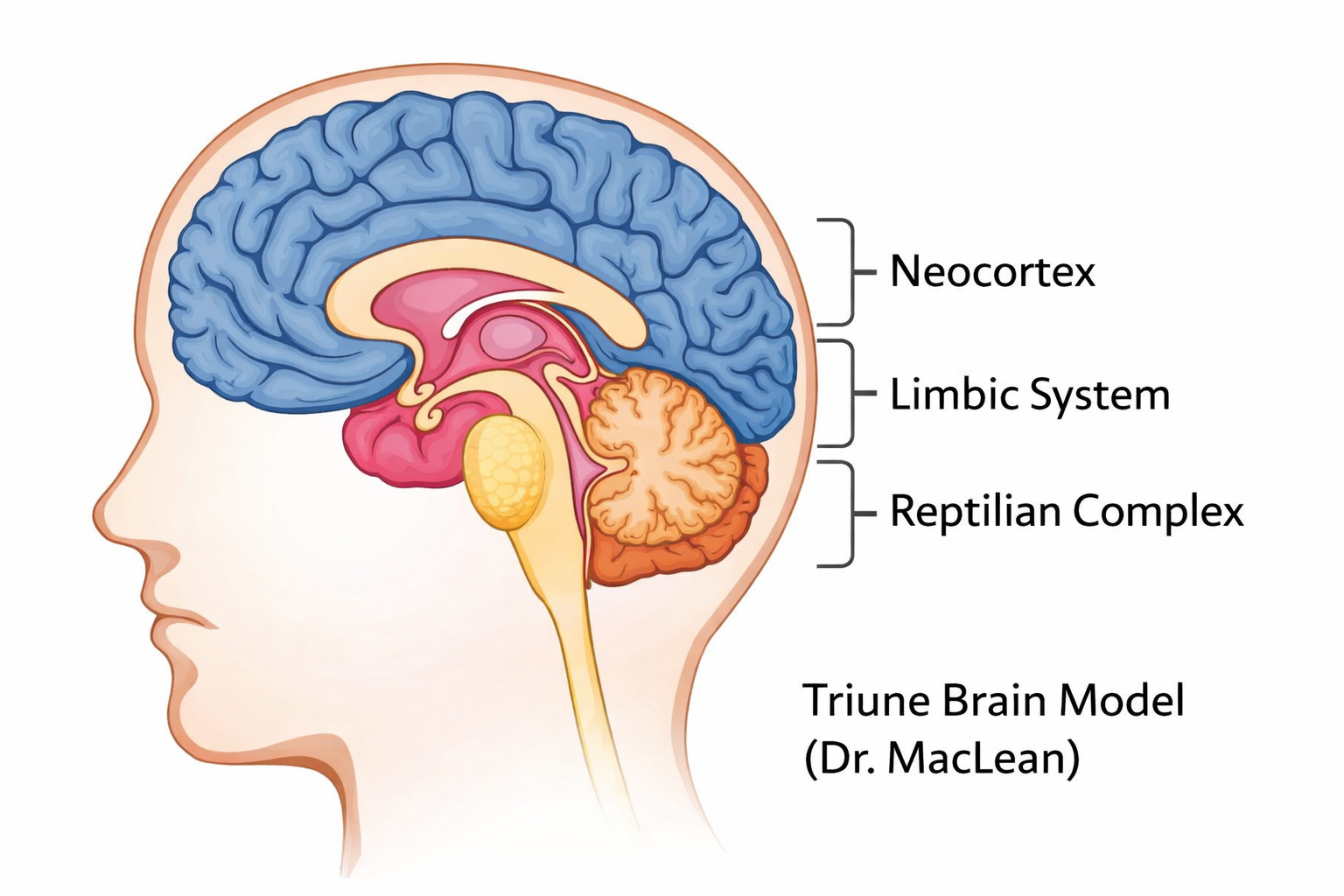
Image Description: The triune brain is schematised in an anatomical figure, which shows the top portion of the cerebral structure (the neocortex), the central part of the brain, where the amygdala is located (the limbic system), and the bottom part of the brain, where the cerebellum can be found (reptilian complex).
Credit: Chat GPT
Lisa Feldman Barrett, Professor of Psychology at Northeastern University, describes the origins of the triune brain in Plato’s philosophy, in which the idea of two horses representing one’s instincts and emotions being controlled by a charioteer — whose representation of rationality controlled them both — laid out the metaphoric basis for an initial explanation of the human brain’s structure and function. Modern neuroscience, however, has largely moved past this model, showing that the brain does not neatly separate function by region in the way MacLean proposed.
So where does that leave Polyvagal Theory?
Polyvagal Theory (PVT), developed by neuroscientist Dr. Stephen Porges in 1994, took a different and more nuanced approach. Rather than focusing on brain regions, Porges turned his attention to the autonomic nervous system — specifically the vagus nerve — and proposed a hierarchical model of how the nervous system responds to safety and threat.
At its core, PVT describes three physiological states: the ventral vagal state (associated with social engagement, calm, and connection), the sympathetic state (fight or flight), and the dorsal vagal state (shutdown or freeze). The theory suggests that our nervous system is constantly scanning the environment for cues of safety or danger — a process Porges calls neuroception — and shifts between these states accordingly, largely below the level of conscious awareness.
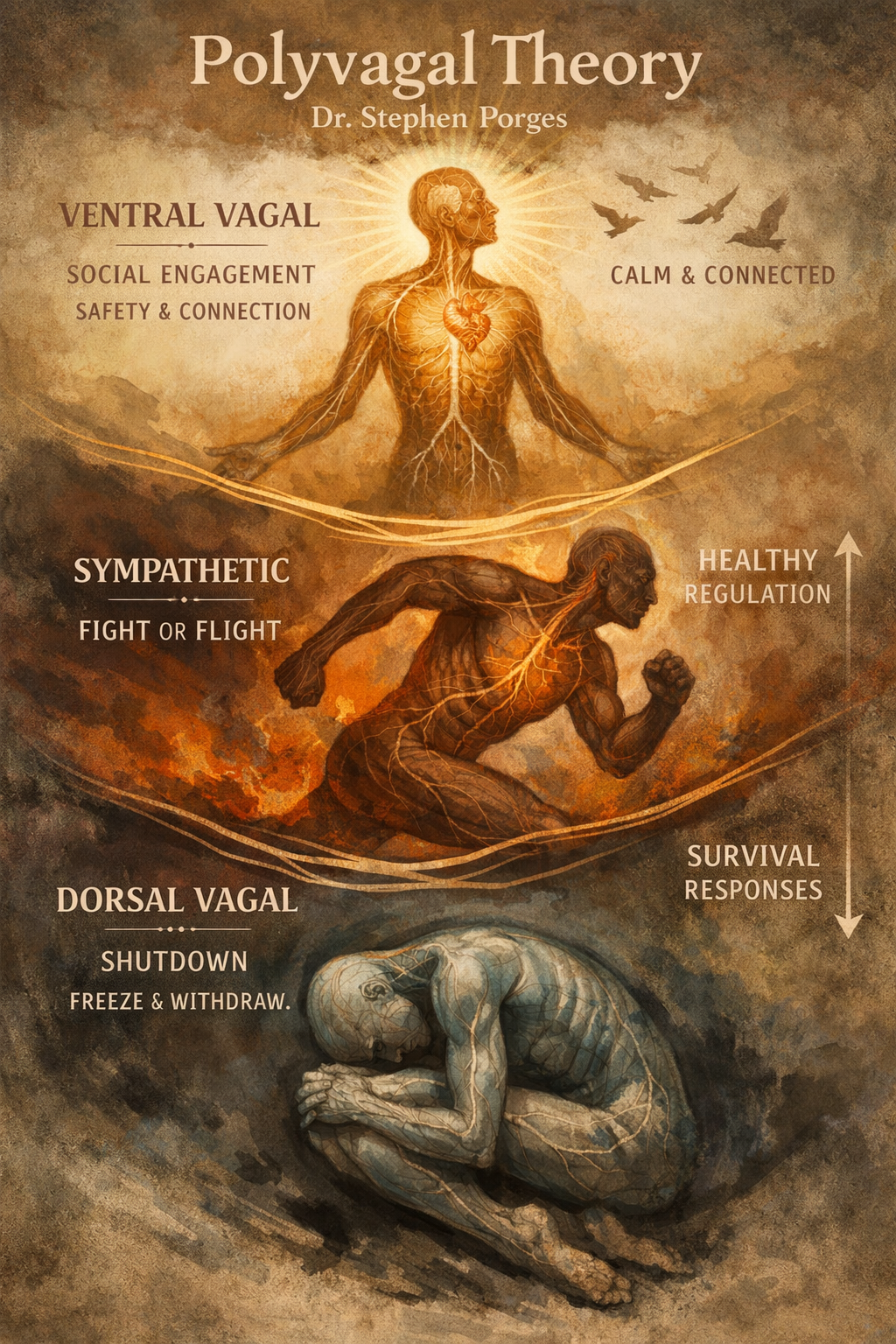
Image Description: An imagetic representation of the Polyvagal Theory shows three humanoid figures, each representing one of the vagal systems. From top to bottom: Ventral Vagal is seen in a bright and sunny human-like representation, standing for social engagement and safety & connection; in the middle, a humanoid seen in movement represents the sympathetic system and the “fight or flight” reaction; at the bottom, the Dorsal Vagal is represented by a human-like figure in a coiled up position, to depict the shutdown state, as well as the shutdown state observed in survival responses.
Credit: Chat GPT
The 2026 criticism — and Porges’ response
A scientific publication in early 2026 challenged several of PVT’s anatomical claims, particularly regarding the myelination of the vagus nerve and whether the evolutionary hierarchy Porges describes holds up under scrutiny. Critics argued that some of the neuroanatomical foundations had been overstated, and that PVT had been embraced by clinicians and somatic practitioners faster than the empirical evidence warranted.
Porges himself responded directly, acknowledging the limitations of any evolving theory while standing firmly behind the model’s clinical relevance and core principles. He has consistently noted that PVT was never intended as a fixed anatomical claim, but rather as a framework for understanding how the body’s state influences behaviour, perception, and connection — a distinction that matters enormously in therapeutic settings.
Why Polyvagal Theory still matters
Here’s the thing: the debate around PVT’s neuroanatomical precision does not erase its practical and clinical value — and this distinction is worth sitting with.
Therapists, somatic practitioners, trauma specialists, and body-based educators have found PVT to be one of the most coherent and compassionate frameworks for understanding human responses to stress and trauma. It offers a language for why someone might freeze in a difficult situation without choosing to, why social connection is genuinely regulating for the nervous system, and why safety — not just cognitive reframing — is the true foundation of healing.
The theory has given both practitioners and clients a way to stop pathologising normal responses. When someone understands that their shutdown or hypervigilance is not a character flaw but a nervous system response shaped by evolution, something shifts. There is less shame, more curiosity, and more room for genuine healing.
Polyvagal Theory and autism: a transformative application
Perhaps one of the most compelling demonstrations of PVT’s real-world value lies in its application to children on the autistic spectrum. When Porges speaks about individuals on the spectrum, he frames it through the lens of physiological state regulation: the autistic body is often locked in a defensive physiological state, and the central question becomes whether we can provide cues that re-tune the autonomic nervous system — enabling the child to spontaneously engage, to hear the human voice against background noise, and to explore the world with greater ease.
This insight led Porges to develop a concrete therapeutic intervention: the Safe and Sound Protocol (SSP). The SSP is a non-invasive, sound-based treatment that uses specially filtered music to stimulate and regulate the vagus nerve. Delivered typically over five to ten hours of listening sessions, it is designed to help reset the nervous system — shifting individuals from states of hyperarousal or shutdown into a more balanced state of safety and social engagement. The SSP rehabilitates middle ear muscle function using music filtered to the specific frequency range of human speech, addressing one of the core sensory challenges experienced by many autistic individuals: auditory hypersensitivity and difficulty processing speech in noisy environments.
The results have been documented across peer-reviewed studies. A 2014 study led by Porges found that the polyvagal-informed intervention could successfully reduce auditory hypersensitivities in people with ASD, and a 2023 study highlighted the SSP as a promising intervention for reducing sensory sensitivities, digestive problems, and selective eating in individuals with autism. Two peer-reviewed studies involving 292 children with ASD who used an early version of the SSP reported significant improvements in emotional organisation, listening, spontaneous speech, and hearing sensitivities.
The case of Sophie, a six-and-a-half-year-old girl diagnosed with ASD, offers a human face to this data. Before the SSP, Sophie was extremely anxious and seemed constantly in a state of threat — her fear prevented her from attempting many things and her over-aroused sympathetic nervous system affected her learning, her speech, and her ability to communicate. After completing the protocol, her mother noted a marked decrease in fear, a more relaxed facial expression, a dramatic improvement in spontaneous language, and the emergence of prosocial behaviour.
What makes this particularly meaningful is how PVT reframes the therapeutic goal: rather than placing intentionality on the individual child — essentially asking them to try harder — the framework recognises that behaviour emerges from physiological state. When the nervous system is dysregulated, the range of accessible behaviour narrows. When it is regulated, the door opens. This is not normalisation. It is liberation — giving children and families more access to life, connection, and joy.
Even if future research refines or revises some of PVT’s anatomical claims, the framework’s invitation — to listen to the body, to cultivate felt safety, and to understand connection as a biological need — is unlikely to lose its relevance. Science is iterative, and good frameworks evolve. The conversation Polyvagal Theory started about the body’s role in emotional regulation and trauma recovery is one that needed to happen, and it continues to ripple through clinical practice, education, and even the performing arts.
For those of us who work with voice, breath, and presence — as singers, actors, or movement practitioners — the polyvagal lens remains one of the most useful tools we have. Understanding how a performer’s nervous system state affects vocal freedom, breath support, and authentic expression is not a metaphor. It is physiology. And that is worth building on, whatever refinements lie ahead.